Background: Anomalous origin of the left coronary artery from the pulmonary artery (ALCAPA) is a rare but life-threatening congenital coronary anomaly that may present with myocardial ischemia, left ventricular dysfunction, mitral regurgitation, and heart failure in infancy. Surgical repair aims to restore a dual-coronary circulation and is usually associated with gradual myocardial recovery. However, patients with severe preoperative instability may develop complex postoperative complications, including persistent ventricular dysfunction, thrombus formation, neurological injury, and multisystem deterioration.
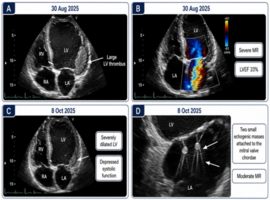
Case Presentation: We report a pediatric patient with ALCAPA managed at a tertiary cardiac center in Riyadh, Saudi Arabia. The patient required extracorporeal membrane oxygenation on 26 August 2025 because of severe cardiorespiratory compromise and subsequently underwent ALCAPA repair on 28 August 2025, with ECMO decannulation on the same day. Delayed sternal closure was performed on 30 August 2025. Early postoperative echocardiography demonstrated severe left ventricular dysfunction with an ejection fraction of 33%, severe mitral regurgitation, and a large left ventricular thrombus. The thrombus was treated with enoxaparin and showed interval improvement. However, the postoperative course remained stormy, complicated by seizures controlled with antiepileptic medications, hypoxic–ischemic encephalopathy, and suspected thromboembolic neurological injury. Brain CT on 6 October 2025 showed hypoxic–ischemic changes involving the basal ganglia and thalami, with pineal region hemorrhage. Subsequent CT on 11 October 2025 demonstrated cortical laminar necrosis. MRI on 13 October 2025 showed generalized brain atrophy, an old left frontoparietal ischemic insult, and scattered small hemorrhagic foci. Respiratory complications included three failed extubation trials, left lower lobe collapse, focal narrowing of the left main bronchus, and bilateral reactive small airway disease. The course was further complicated by resolved fungal and Serratia marcescens infections. The patient sustained cardiopulmonary arrest requiring 4 minutes of CPR on 8 October 2025 and died on 15 October 2025 after prolonged CPR lasting 36 minutes.
Conclusion: This case highlights a severe postoperative neurocardiac cascade after ALCAPA repair, linking persistent ventricular dysfunction, intracardiac thrombosis, hypoxic–ischemic brain injury, cortical laminar necrosis, respiratory failure, and mortality. It emphasizes the need for vigilant postoperative echocardiographic, neurological, respiratory, and anticoagulation surveillance in high-risk pediatric ALCAPA patients.
Keywords: ALCAPA; Cortical laminar necrosis; Intracardiac thrombus; Hypoxic–ischemic encephalopathy; Pediatric cardiac surgery; Postoperative complications; Left ventricular dysfunction; Case report