Wajeeh ur Rehman1*, Shiau-Ing Wu1, Nabil Braiteh2, Owais Ahmed2 and Hisham Kashou2
1United Health Services Hospitals, Wilson Regional Medical Center, Department of Internal Medicine, NY, USA
2United Health Services Hospitals, Heart and Vascular Institute, Wilson Regional Medical Center, Department of Cardiology and Cardiovascular surgery, NY, USA
*Corresponding author: Wajeeh ur Rehman, United Health Services Hospitals, Wilson Regional Medical Center, Department of Internal Medicine, NY, USA.
Received: June 22, 2023; Accepted: July 05, 2023; Published: July 18, 2023
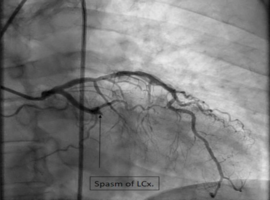
Citation: Rehman Wu, Wu SI, Braiteh N, et al. A Rare Case of ST Elevation with Complete Occlusion of the Left Circumflex Artery in the Setting of Anaphylactic Shock: A Case Report. Case Rep Clin Cardiol J. 2023; 3(3): 134.